I en studie av Michael Thun uppmärksammades att cigaretter blivit allt giftigare i så motto att kroniska rökare drabbades oftare och svårare av ”modernare” cigaretter än de som såldes på 1950- och 1960-talet. Självklart har produktutvecklingen inte stått stilla hos tobaksindustrin, men att driva utvecklingen mot allt skadligare produkter är verkligen häpnadsväckande. Thun och medarbetare skriver:
Bakgrund
Sjukdomsriskerna från cigarettrökning ökade i USA under större delen av 1900-talet, först bland manliga rökare och senare bland kvinnliga rökare. Huruvida dessa risker har fortsatt att öka under de senaste 20 åren är oklart.
Metoder
Vi mätte tidsmässiga trender i dödlighet över tre tidsperioder (1959–1965, 1982–1988 och 2000–2010) och jämförde absoluta och relativa risker baserat på kön och självrapporterad rökstatus i två historiska kohortstudier och i fem poolade samtida kohortstudier, bland deltagare som blev 55 år eller äldre under uppföljningen.
Resultat
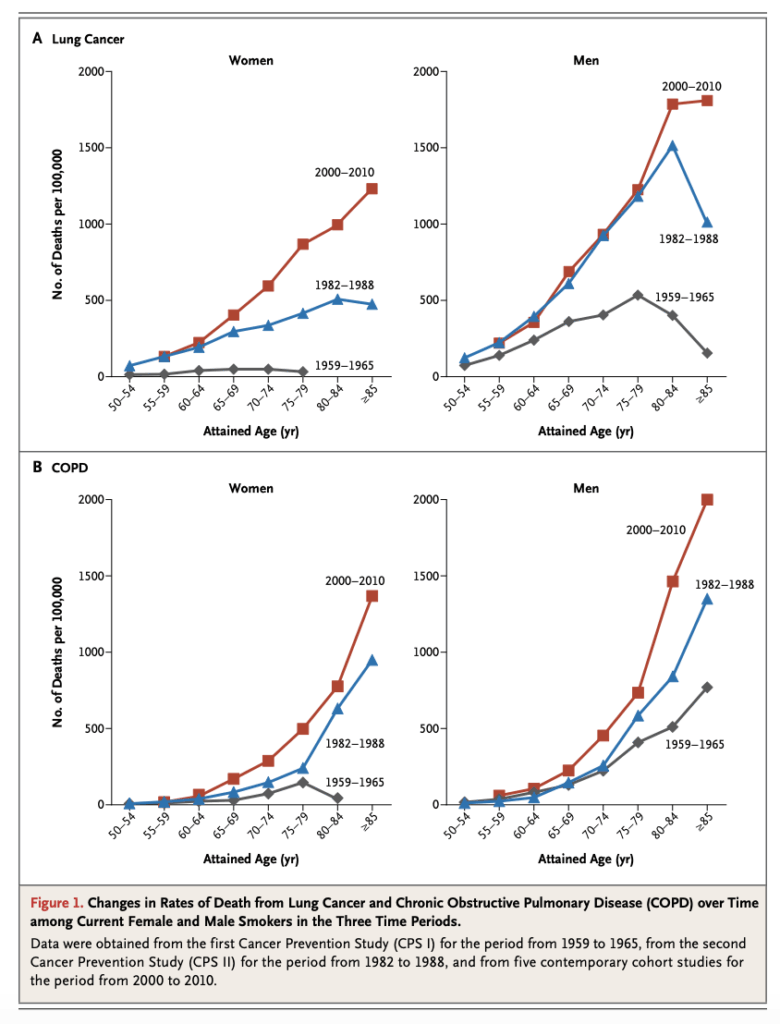
För kvinnor som var nuvarande rökare, jämfört med kvinnor som aldrig hade rökt, var de relativa riskerna för död i lungcancer 2,73, 12,65 respektive 25,66 på 1960-, 1980- respektive samtida kohorter; Motsvarande relativa risker för manliga rökare, jämfört med män som aldrig rökt, var 12,22, 23,81 och 24,97. I de samtida kohorterna hade manliga och kvinnliga rökare också liknande relativa risker för dödsfall i kroniskt obstruktiv lungsjukdom (KOL) (25,61 för män och 22,35 för kvinnor), ischemisk hjärtsjukdom (2,50 för män och 2,86 för kvinnor), alla typer av stroke (1,92 för män och 2,10 för kvinnor) och alla orsaker tillsammans (2,80 för män och 2,76 för kvinnor). Dödligheten i KOL bland manliga rökare fortsatte att öka i de samtida kohorterna i nästan alla åldersgrupper som representerades i studien och inom varje stratum av rökningens varaktighet och intensitet. Bland män i åldern 55 till 74 år och kvinnor i åldern 60 till 74 år var totalmortaliteten minst tre gånger så hög bland nuvarande rökare som bland dem som aldrig rökt. Rökstopp oavsett ålder minskade dödligheten dramatiskt.
Slutsatser
Risken för dödsfall från cigarettrökning fortsätter att öka bland kvinnor och de ökade riskerna är nu nästan identiska för män och kvinnor, jämfört med personer som aldrig har rökt. Bland män har riskerna i samband med rökning planat ut på de höga nivåerna som sågs på 1980-talet, förutom en fortsatt, oförklarlig ökning av dödligheten från KOL.
Thun MJ, Carter BD, Feskanich D, Freedman ND, Prentice R, Lopez AD, Hartge P, Gapstur SM. 50-year trends in smoking-related mortality in the United States.
N Engl J Med. 2013 Jan 24;368(4):351-64. doi: 10.1056/NEJMsa1211127.
PMID: 23343064 Free PMC article.